Презентація на тему:
goiter
Завантажити презентацію
 KFCH")



 true fibrous capsule: enveloping the gland. 2)false fascial caps...")

sup.thyroid artery :branch of external carotid a ,closely...")
sup.thyroid v .from apex to I.j.v 2)middle thyroid v from...")
as...")










is d...")








 Close...")
close follow up till fully consciouss 2)at bed side clip remover in case of...")
hemorrage :occur due to sliped either ligature of superior thyroid artery o...")
recurrent laryngeal nerve palsy: May be unilateral or bilateral Unilateral:...")
hypoparathyroidism : Rarely complication Temporary due to vascular spasm of...")
: Occur in thyrotoxic patient not well prepa...")




goiter
Завантажити презентаціюПрезентація по слайдам:
 KFCH")
Dr :Talal Mgboul R(3) KFCH

. Definition . Surgical Anatomy . Thyroidectomy . Types . Pre op preparation . Anasthesia . Procedure . Post op management . Complications

Thyroid gland : is endocrine gland situated in mid line of neck against vertebra C 5-6-7 T1. Weight about 20-25g. Shape : butter fly formed of 2 lateral lobes connected by an ithmus.

Anatomy : Each thyroid lobe is pear shaped with it is apex reaching oblique line of thyroid cartilage . The isthmus crosses the 2nd ,3rd ,4th tracheal ring and may project upwards forming the pyramidal lobe which connected to hyoid bone by fibrous band.
 true fibrous capsule: enveloping the gland. 2)false fascial caps...")
Capsules: 1) true fibrous capsule: enveloping the gland. 2)false fascial capsule :derived from pretracheal fascia which attached above thyroid cartilage &hyoid bone so it allow the gland to move up during deglutition. The fascia is thickened posteriorly forming the ligament of berry which fixes the back of the gland to cricoid cartilage.

Medially :each lobe moulded over larynx and trachea. Superiorly: the gland over lies cricothyroid muscle . External branch of superior laryngeal nerve pass deep to upper pole of thr gland on it is way to supply muscle. Posterolaterally: contact with carotid sheath and parathyroid. Posteriomedially :related to tracheooesophageal groove in which run recurrent laryngeal nerve.
sup.thyroid artery :branch of external carotid a ,closely...")
Arterial supply : 1)sup.thyroid artery :branch of external carotid a ,closely related to external laryngeal nerve but separate it close to the apex of the gland. 2)inf thyroid artery :branch of thyrocervical trunk of subclavian artery ,it is terminal branches related to R.laryngeal nerve close to the gland. 3)thyroid ima artery :(may be absent)arise from arch of aorta or innominate a .&ascend in front of trachea to reach the isthmus.
sup.thyroid v .from apex to I.j.v 2)middle thyroid v from...")
Venous drainaige: 1)sup.thyroid v .from apex to I.j.v 2)middle thyroid v from base to i.j.v 3)inf thyroid vein from isthmus to innominate vein.
as...")
Definition: it is aremoval of all or part of thyroid gland Indications : A)as therapy for patient with thyrotoxicosis. B)to treat benign or malignant thyroid tumor. C)to treat pressure symptoms such as respiratory disetress or dyspnea or dysphagia. D)cosmotic purpose. E)To establish difinitive treatment of thyroid mass specially when cytological results is indetermenate.

Hemithyroidectomy Subtotal thyroidectomy Near total thyroidectomy Total thyroidectomy

It involve removal of one lobe plus entire isthmus is removed. It is performed in benign didease involving one lobe. Also done in follicular carcinoma involving one lobe. Other indication: A)solitary toxic or non toxic nodule . B)thyroid cyst.

Here about 8 gm ,or tissue size of pulp of finger is retained on lower pole of thyroid on both sides ,and rest of gland is removed. Indications: Toxic thyroid (primary or secondary) Non toxic multinodular goitre.

Here both lobes except less than 2gm of thyroid tissue on the lower pole,near to the recurrent laryngeal nerve and parathyroid ,are removed to retain blood suplly to parathyroid gland . Indication : mostly done in papillary thyroid carcinoma .

Here entire gland is removed. Indication: Follicular thyroid cancer Papillary thyroid cancer

Blood group and cross matching keep required blood ready. Indirect laryngoscope:check for abduction of vocal cord. Serum calcium estimation because hyperparathyroidism may coexcist. T3 ,T4, TSH. Thyroid antibodies. ECG & cardiac fitness specially in cases of toxic goitre. Lugol,s iodine is given 10days prior to surgery to make the gland firm and less vascular.

Scar Airway obstruction Voice change Hypothyroidism Hypoparathyroidism

Position: under general anasthesia patient is put on supine position,with nech hyperextended with sandbag under shoulder ,table tilt 15degree head to reduce venous congestion.(rose position) skin is prepped from chin to the upper thorax. surgeon and assistant scrup and gown the stand the opposite site. usually start the larger gland first.

Site of incision is identified with suture. Transverse skin crease incision is placed 2-3 cm above the sternal notch about 8cm long extending to lateral border of sternocleidomastoid muscle. The scapel with size 15 blade is slanted to divide skin and platysma. Hemostasis controlled with electrocuttary.

Subcutanous tissue and platysma are incised in platysmal plane ,remaining superfecial to anterior jugular vein. Upper flap rised up to thyroid cartilage. Lower flap up to sternoclavicular joint. deep fascia is opened vertically in mid line.
is d...")
The fascia between strap muscles (sternohyoid,sternothyroid,and omohyoid)is divided,along midline and muscle retracted laterally. In case of larger goitre or any neoplasm strap muscle devided in upper part .

It cover the thyroid gland Is opened vertically to expose the thyroid gland.

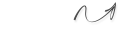
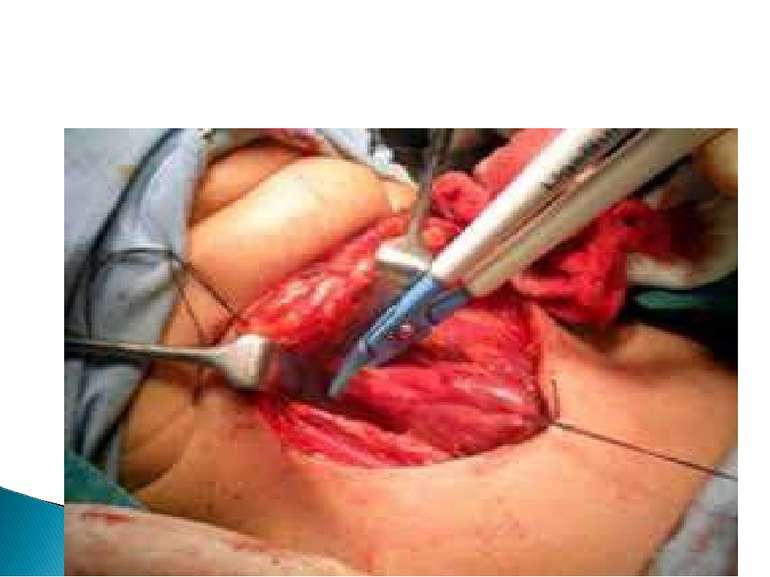
The thyroid gland is rotated medially using surgeon finger . The middle thyroid vein identified which is then ligated. This permit further mobilization of the gland.

Superior pole is dissected Identify the superior thyroid artery, close to superior pole of the thyroid paranchyma and ligate it. Dissection is done in avascular plane between upper pole of the gland and cricothyroid muscle to avoid trauma of external branch of superior laryngeal nerve entering cricothyroid.

Location:in the posterior position at the level of upper 2/3 of the thyroid and approximately 1cm above and behind the crossing point of recurrent laryngeal nerve and inferior thyroid artery. It is orange yellow in colour. The gland must remain in situ with blood supply intact.

Location :between lower pole of thyroid and isthmus,below and in front of crossing . Care must be give to preserve it in situ to avoid damage it is inferior thyroid artery supplying both glands.

It is abranch of thyrocervical trunk . Ligation done at capsular level,at the lower pole of thyroid gland. It retain blood supply of parathyroid very importand.

Should be identified with dissection of entire course . Recurrent laryngel nerve is located in Riddles triangle Sup:inf thyroid artery Med trachea Lateral:common carotid artery

Berrys ligament :define the posteriolateral attachment of thyroid gland . Plunt dissection can be used to further expose this fascia ,then with scalpel transect the ligament. Offten minimal amount of thyroid tissue left near the entrance of recurrent laryngeal nerve into the larynx to reduce risk of injury.
 Close...")
Absolute hemostasis Suction drain to thyroid bed (beneath strap muscle) Close loosely in layer with absorbable sutures. Close skin with suture or clips Check vocal cord on extubation by direct laryngoscope.
close follow up till fully consciouss 2)at bed side clip remover in case of...")
1)close follow up till fully consciouss 2)at bed side clip remover in case of respiratory distress. 3)calcium gluconate in case of acute hypocalcemia. 4)remove : Drain :when dry 24-48hours post operativly Sutures 3-5days post operativly
hemorrage :occur due to sliped either ligature of superior thyroid artery o...")
1)hemorrage :occur due to sliped either ligature of superior thyroid artery of small veins. It causes tachycardia,hypotension,breathlessness,severe stridor. Treatment:ligation of bleeder under general anasthesia. 2)respiratory obstruction: occur due to: Hematoma laryngeal edema (commonest) bilateral recurrent nerve palsy Treatment :evacuation of hematoma
recurrent laryngeal nerve palsy: May be unilateral or bilateral Unilateral:...")
3)recurrent laryngeal nerve palsy: May be unilateral or bilateral Unilateral: mostly asymptomatic only some change in voice which gradually become normal ,no need specific treatment. Bilateral: change in voice and severe dyspnea and stridor lead to respiratory arrest . Treatment :emergency tracheostomy.
hypoparathyroidism : Rarely complication Temporary due to vascular spasm of...")
4)hypoparathyroidism : Rarely complication Temporary due to vascular spasm of parathyroid gland . Occur in 2nd to 5th post operative day. It present with muscle weakness and convulsion Tratment is calcium gluconate iv 8 hourly Later oral calcium supplement.
: Occur in thyrotoxic patient not well prepa...")
Thyrotoxic crises (thyroid storm): Occur in thyrotoxic patient not well prepared for surgery Other causes infection, DM, pre_eclampsia. Features: Severe dehydration,circulatory collpse,hypotension,hyperpyrexia. Tachypnea,palpiatation,cardiac failure. GIT :vomiting or diarrhea.

Rised T3,T4,Calcium Change in ECG, cardiography ,ABG. TREATMENT : Fluid therapy,cold sponge,iv paracetamol. Iv hydrocortisone 500mg. Propranol 80mg orally (very important). Cholestramine. Digoxin in case of cardiac failure. Hemodialysis,plasmapheresis,exchange transfusion.

External laryngeal nerve injury. Hypothyroidism. Recurrent thyrotoxicosis. Wound infection and stitch site granuloma formation. Keloid scar.

Baily and love . Google .com. Dr sameh doss surgial anatomy. Kasr alaini text book.

Схожі презентації
Категорії