Презентація на тему:
Pharmacogenetic_lecture2
Завантажити презентацію






 SNPs are single base pair positions in...")
 SNPs are very common in the human popu...")
 Tandem Repeat Polymorphism...")
 Insertion/Deletion Polymor...")







 Phar...")
Pharmacogenetic_lecture2
Завантажити презентаціюПрезентація по слайдам:

Pharmacogenetics/Pharmacogenomics

Outline Introduction Differential drug efficacy People react differently to drugs Why does drug response vary? Potential causes of variability in drug effects Genetic variation Pharmacogenetics What is Pharmacogenetics? Pharmacogenetics VS. Pharmacogenomics Genetic variation and drug response Determinants of Drug Efficacy and Toxicity Examples

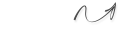
Differential drug efficacy Same symptoms, Same findings, Same disease? Same drug Same dose Different patients At a recommended prescribed dosage— a drug is efficient in most. not efficient in others. harmful in a few. Lack of efficacy Unexpected side-effects

Patient population with same disease phenotype Patients with normal response to drug therapy Patients with non-response to drug therapy Patients with drug toxicity “One size does not fit all …” People react differently to drugs Ethnicity Age Pregnancy Genetic factors Disease Drug interactions


Genetic variation Why does drug response vary?

Genetic variation Primarily two types of genetic mutation events create all forms of variations: Single base mutation which substitutes one nucleotide for another --Single nucleotide polymorphisms (SNPs) Insertion or deletion of one or more nucleotide(s) --Tandem Repeat Polymorphisms --Insertion/Deletion Polymorphisms Polymorphism: A genetic variation that is observed at a frequency of >1% in a population
 SNPs are single base pair positions in...")
Single nucleotide polymorphisms (SNPs) SNPs are single base pair positions in genomic DNA at which different sequence alternatives (alleles) exist wherein the least frequent allele has an abundance of 1% or greater. SNP might change the DNA sequence SNPs are the most commonly occurring genetic differences.
 SNPs are very common in the human popu...")
Single nucleotide polymorphisms (SNPs) SNPs are very common in the human population. Between any two people, there is an average of one SNP every ~1250 bases. Most of these have no phenotypic effect estimate that 3.2 million SNPs in genome only
 Tandem Repeat Polymorphism...")
Insertion or deletion of one or more nucleotide(s) Tandem Repeat Polymorphisms Tandem repeats or variable number of tandem repeats (VNTR) are a very common class of polymorphism, consisting of variable length of sequence motifs that are repeated in tandem in a variable copy number. Can affect transcript amount Based on the size of the tandem repeat units: Microsatellites or Short Tandem Repeat (STR) repeat unit: 1-6 (dinucleotide repeat: TATA- in UCIT1A1 (glucuronosil transferase) promoter) Minisatellites repeat unit: 14-100
 Insertion/Deletion Polymor...")
Insertion or deletion of one or more nucleotide(s) Insertion/Deletion Polymorphisms Insertion/Deletion (INDEL) polymorphisms are quite common and widely distributed throughout the human genome Larger insertions/deletions that add or substract amino acids (CBS-Cystathionine β-synthase, common 68 bp INDEl polymorphism which affect folate level) Gene duplication – stably transmitted inherited germline gene replication that causes increased protein exp. and activity (CytochromeP4502D6, up to 13 genes) Large Deletions – gene deletions, result in complete loss of protein production (entire GSTM1-glutathione-S-transferase, homozygous null individuals have only 50% of glutathione conjugating capacity of those with at least one copy of the gene)

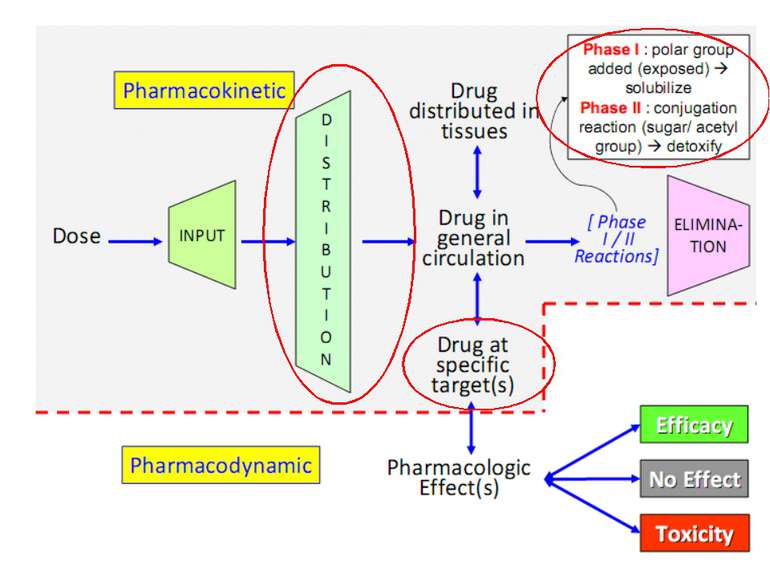
Pharmacokinetics and Pharmacodynamics
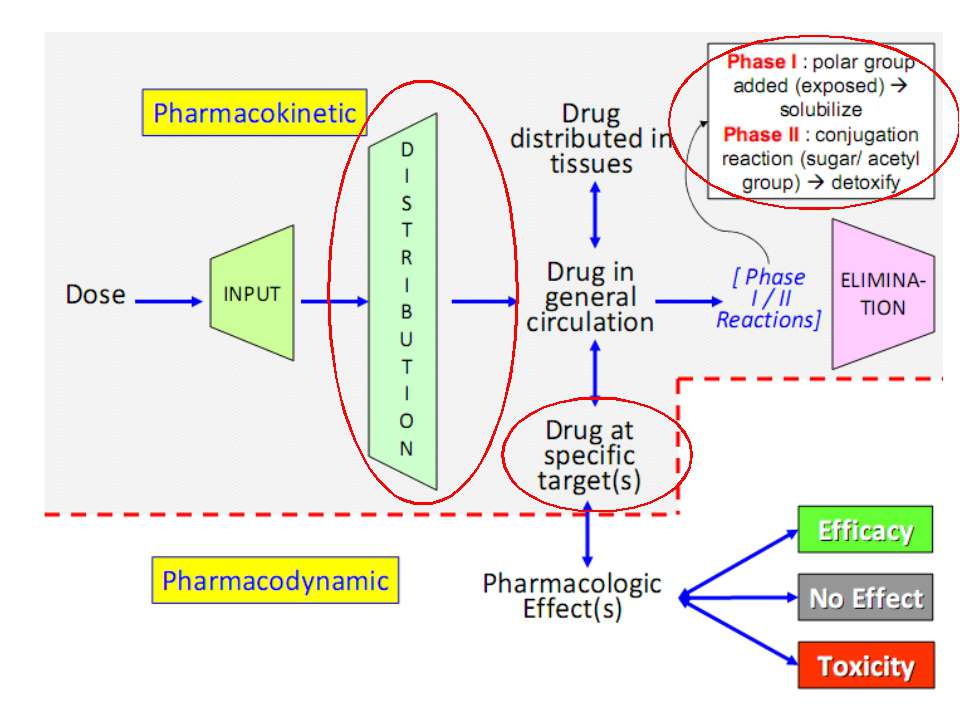

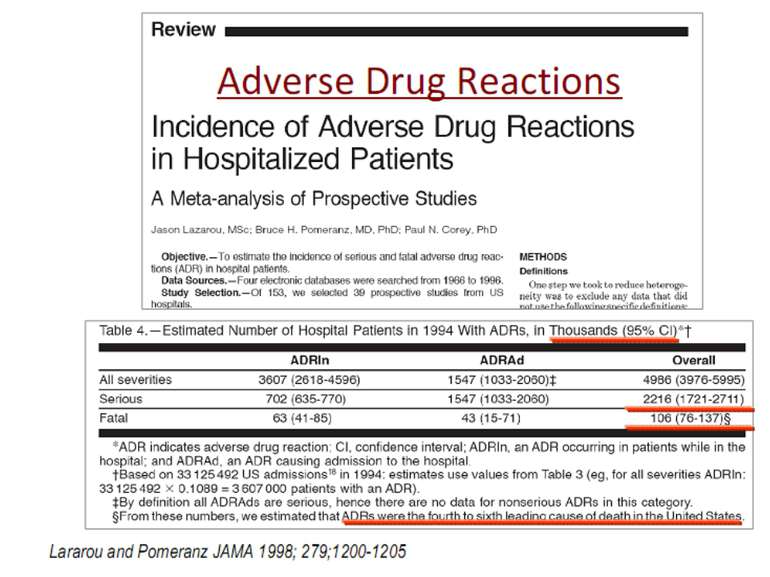
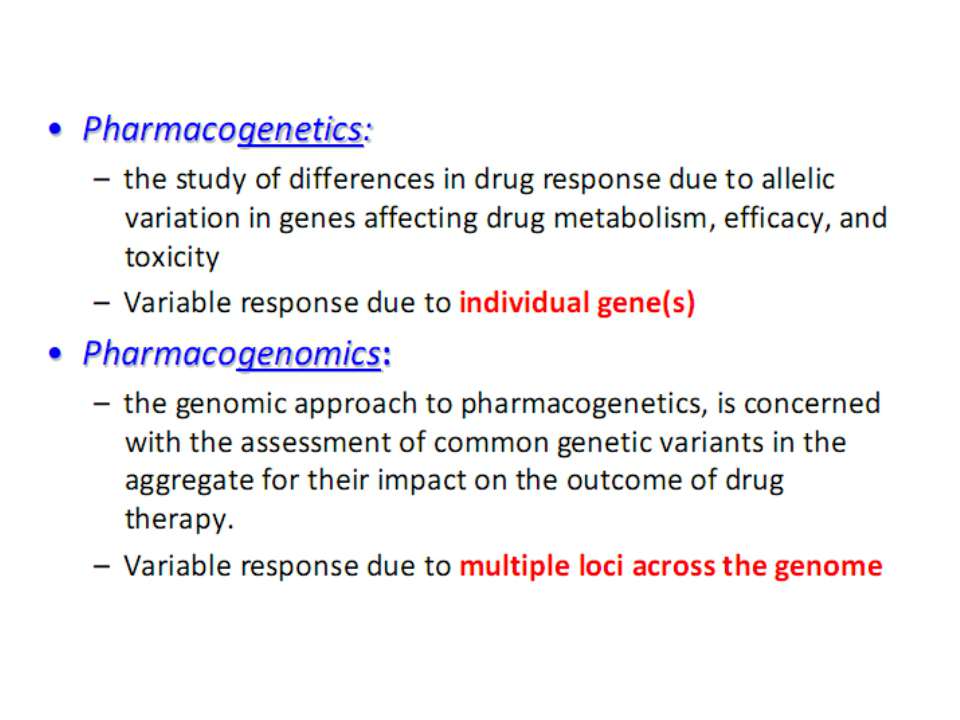
Pharmacogenetics The study of variations in genes that determine an individual’s response to drug therapy. Common variation in DNA sequence (i.e. in >1% of population) Genetic Polymorphism: SNPs; INDEL; VNTRs Potential Target Genes are those that encode: Drug-metabolizing enzymes Transporters Drug targets

Example


A simple test, the urinary metabolic ratio, after administration of a probe drug can identify the extensive metabolizer and the poor metabolizer phenotype

CYP2D6 THE DEBRISOQUINE-SPARTEINE POLYMORPHISM 1977, physicians at St. Mary’s Hospital Medical School in London – a volunteer’s hypotensive response to debrisoquine, a sympatholytic antihypertensive drug, was markedly increased because of impaired metabolism. Group of Germany physicians independently observed increased side effects associated with decreased oxidative metabolism of sparteine, an alkaloid drug with antiarrhythmic actions . Family studies revealed that both oxidative metabolic reactions are under monogenic control and that poor metabolizers are homozygous for a recessive allele. A simple test, the urinary metabolic ratio (MR) →5 to 10% of individuals in white populations are of the poor-metabolizer phenotype, compared with only 1 to 2% in Asian populations
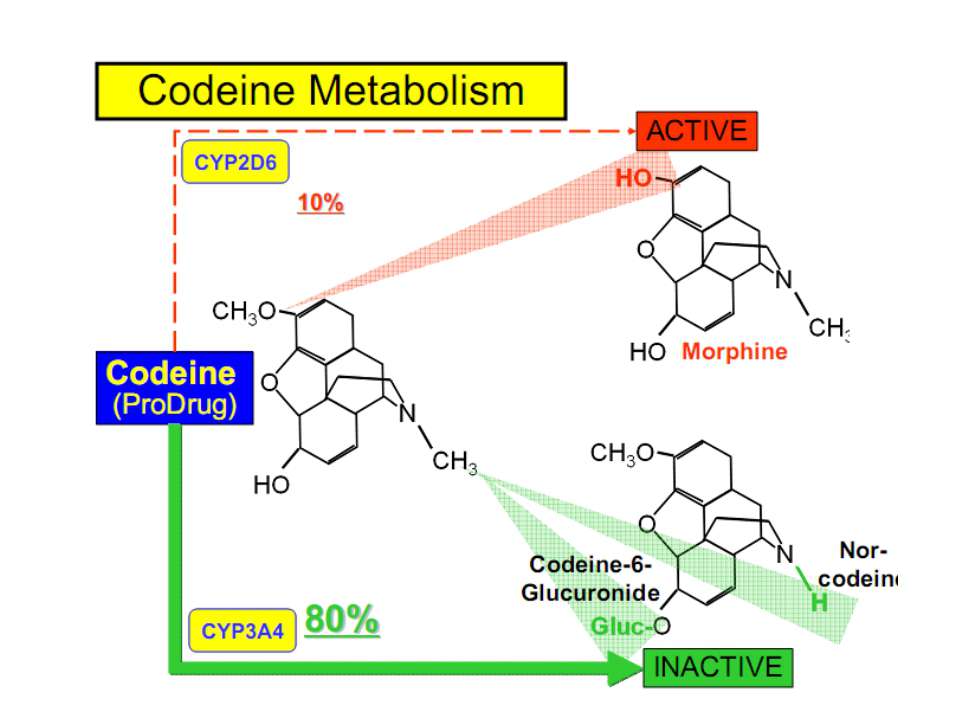

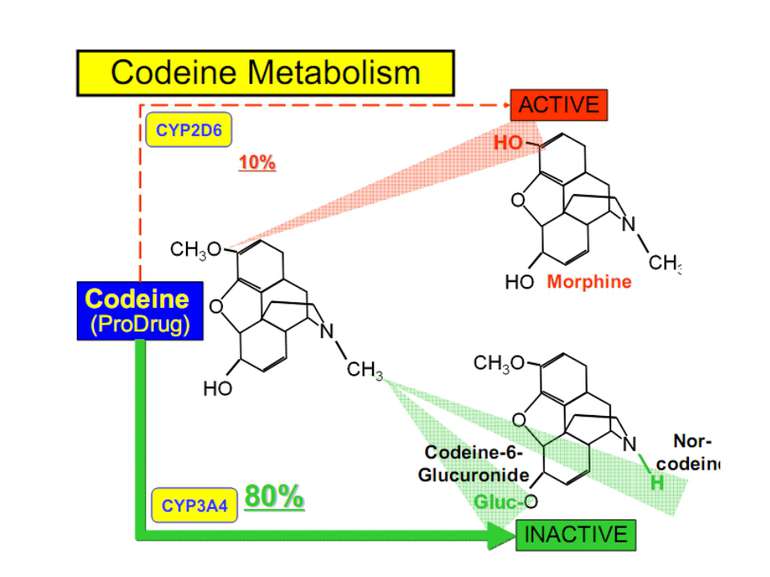
CONSEQUENCES OF THE DEFICIENT CYP2D6 Responsible for metabolism of 15-25% of all medicines in use Poor-metabolizer (7 variants of low-activity alleles) Increased risk of toxicity of antidepressants or antipsychotics (catabolized by the enzyme drugs) 2. Lack of analgesic effects of codeine (anabolized by the enzyme) 3. Exaggerated response to Ultra-rapid-metabolizer (stable gene duplication, up to 13 active genes) 3. Extremely rapid clearance and thus inefficacy of antidepressants

Pharmacogenetics in Clinical Practice 20-40% of patients benefit from an approved drug 70-80% of drug candidates fail in clinical trials Many approved drugs removed from the market due to adverse drug effects The use of DNA sequence information (genome-wide approach) to measure and predict the reaction of individuals to drugs. Personalized drugs Faster clinical trials Less drug side effects
 Phar...")
WWW.PHARMGKB.ORG (NIH Sponsored Research Network And Knowledge Database) Pharmacogenetics and Pharmacogenomics Knoweledge Base (PharmGKB) Genotype and phenotype data related to drug response
Схожі презентації

Категорії